English name: Imatinib Mesylate Tablets
Chinese Pinyin: Jiahuangsuan Yimatini Pian
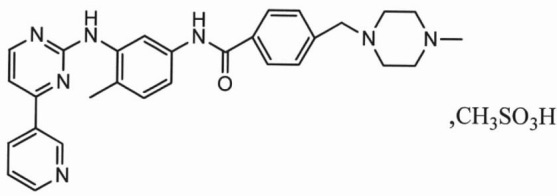
The main ingredient of this product is imatinib mesylate.
Chemical name: 4-[(4-methyl-1-piperazinyl)methyl]-N-[4-methyl-3-[[4-(3-pyridyl)-2-pyrimidinyl]amino] Phenyl]-benzamide methanesulfonate

| 【Name】 | Common Name: Imatinib Mesylate Tablets English name: Imatinib Mesylate Tablets Chinese Pinyin: Jiahuangsuan Yimatini Pian |
|---|---|
| 【Ingredient】 | The main ingredient of this product is imatinib mesylate. Chemical name: 4-[(4-methyl-1-piperazinyl)methyl]-N-[4-methyl-3-[[4-(3-pyridyl)-2-pyrimidinyl]amino] Phenyl]-benzamide methanesulfonate
Molecular formula: C29H31N7O·CH4SO3 Molecular weight: 589.71 |
| 【Description】 | Very dark yellow to brownish orange, film-coated tablets. |
| 【Indication】 | - Chronic, accelerated or blast phase for the treatment of Philadelphia chromosome-positive chronic myelogenous leukemia (Ph+CML); - Adult patients for the treatment of malignant gastrointestinal stromal tumors (GIST) that cannot be removed and/or metastasized; the safety and efficacy information for the following indications mainly comes from foreign research data, and the data of the Chinese population is limited; -Adult patients with relapsed or refractory Philadelphia chromosome positive acute lymphoblastic leukemia (Ph+ ALL) -Adult patients with hypereosinophilic syndrome (HES) and/or chronic eosinophilic leukemia (CEL) who have the FIP1L1-PDGFRα fusion kinase (mutational analysis or FISH demonstration of CHIC2 allele deletion) and for patients with HES and/or CEL who are FIP1L1-PDGFRα fusion kinase negative or unknown. -Adult patients with myelodysplastic/myeloproliferative diseases(MDS/MPD) associated with PDGFR (platelet-derived growth factor receptor) gene re-arrangements. -Adult patients with aggressive systemic mastocytosis (ASM) without the D816V c-Kit mutation as determined or with c-Kit mutational status unknown -Adult patients with unresectable, recurrent and/or metastatic dermatofibrosarcoma protuberans (DFSP). -Patients with Kit (CD117) positive unresectable and/or metastatic malignant gastrointestinal stromal tumors (GIST). |
| 【Strength】 | 0.1g(Calculated on C29H31N7O). |
| 【Dosage and Administration】 | The prescribed dose should be administered orally, with a meal and a large glass of water. Doses of 400 mg or 600 mg should be administered once daily, whereas a dose of 800 mg should be administered as 400 mg twice a day(in the morning and evening). Children and adolescents take it once daily or twice a day (morning and evening). For patients unable to swallow the film-coated tablets(including children), the tablets may be dispersed in a glass of water or apple juice. The required number of tablets should be placed in the appropriate volume of beverage (approximately 50 mL for a 100 mg tablet, and 200 mL for a 400 mg tablet) and stirred with a spoon. The suspension should be administered immediately after complete disintegration of the tablet(s). As long as the patient continues to benefit, the treatment of this product should continue.
Dosage for Ph+CML Adult The recommended dose of imatinib mesylate in the chronic phase is 400 mg/day, and the patient in the blast phase and accelerated phase is 600 mg/day. For first-line treatment of patients with WBC >50000/μl CML, treatment experience is limited to patients who have been treated with hydroxyurea. The treatment may begin with the addition of imatinib mesylate. There are no serious adverse drug reactions and if the blood is approved, the dose may be considered to increase from 400 mg/day to 600 mg/day, or from 600 mg/day to 800 mg/day if: disease progression occurs at any time, treatment is at least 3 months After a satisfactory hematologic response was not obtained, no cytogenetic response was obtained after 12 months of treatment, and the hematological and/or cytogenetic responses that had been obtained disappeared again.
Children and adolescents over 3 years old At present, the clinical data of children at home and abroad is limited, and the efficacy and safety of children should be closely monitored. If necessary, the dosage should be adjusted in time.
The safety and efficacy information of this product for children and adolescents over 3 years old is mainly from foreign clinical research data. According to the adult dose, the recommended daily dose is: the accelerated phase of the chronic phase and the blast phase of 340mg/m2 (the total dose does not exceed 600mg/day) to formulate the daily recommended dose for children, the calculated dose should generally be adjusted up to 100 milligrams. The dose for children under 12 years of age should generally be adjusted up to 50 milligrams. There is no experience in treating children under 3 years of age.
Dosage for Ph+ALL The recommended dose of Imatinib Mesylate is 600 mg/day for adult patients with relapsed/refractory Ph+ ALL.
Dosage for GIST patients The recommended dose of Imatinib Mesylate is 400 mg/day for patients with unresectable and/or metastatic, malignant GIST. A dose increases from 400 mg/day to 600 mg/day or 800 mg/day daily may be considered, as clinically indicated, in patients showing clear signs or symptoms of disease progression at a lower dose and in the absence of severe adverse drug reactions. For patients with GIST, imatinib mesylate should be treated continuously unless the condition progresses. The recommended dose for adjuvant therapy in adult patients after complete GIST resection is 400 mg/day. In clinical studies, imatinib mesylate was administered for 3 years. The recommended duration of treatment is at least 36 months. The optimal duration of adjuvant therapy with imatinib is unclear.
Dosage for HES/CEL patients The recommended dose of this product for HES/CEl treatment is mainly based on the dose reported in foreign studies. For HES/CEL demonstrating the presence of the FIP1L1-PDGFR-α fusion kinase, the recommended starting dose is 100 mg/day. If appropriate reductions are not confirmed after treatment and no adverse reactions occur, consider increasing the 100 mg/day dose to 400 mg/day.
Dosage of ASM patients The recommended dose of this product for ASM treatment is mainly based on the dose reported in foreign studies. The recommended dose of imatinib mesylate is 400 mg/day for adult patients with ASM without the D816V c-Kit mutation. If c-Kit mutational status is not known or unavailable, treatment with imatinib mesylate 400 mg/day may be considered for patients with ASM not responding satisfactorily to other therapies. For patients with ASM associated with eosinophilia, a clonal hematological disease related to the fusion kinase FIP1L1-PDGFRα, a starting dose of 100 mg/day is recommended. Dose increase from 100 mg to 400 mg for these patients may be considered in the absence of adverse drug reactions if assessments demonstrate an insufficient response to therapy.
Dosage for Patients with MDS/MPD The recommended dose of this product for MDS/MPD treatment is mainly based on the dose reported in foreign studies. Determine PDGFRb gene rearrangements status prior to initiating treatment. The recommended dose of imatinib mesylate is 400 mg/day for adult patients with MDS/MPD.
Dosage for Patients with DFSP The recommended dose of this product for DFSP treatment is mainly based on the reported dose of foreign research. The recommended dose of imatinib mesylate is 400 mg/day for adult patients with DFSP. The dose can be increased to 800 mg per day when needed.
Dose Modification after adverse reactions If a serious non-hematologic adverse reaction (such as severe water retention) occurs during the treatment with imatinib mesylate, the drug should be discontinued until the adverse reaction disappears, and then the dose is adjusted according to the severity of the adverse reaction.
Dose Modification for severe hepatotoxicity If bilirubin rises > the upper limit of the normal range is 3 times or the transaminase is increased > the upper limit of the normal range is 5 times, it is advisable to stop taking imatinib mesylate until the above indicators fall below 1.5 or 2.5 times the upper limit of the normal range. Later, imatinib mesylate treatment can be continued after taking the dose. The daily dose for adults should be reduced from 400 mg to 300 mg, or from 600 mg to 400 mg or from 800 mg to 600 mg; children and adolescents reduced from 260 mg/m2 to 200 mg/m2 or from 340 mg/m2 to 260 mg/m2.
Dose Modification for neutropenia or thrombocytopenia Ph+CML accelerated or blast phase, Ph+ALL (starting dose 600mg/day, or 340mg/m2/day for children and adolescents): if severe neutrophils and thrombocytopenia occur (neutrophils <0.5×109) /L and / or platelets <10 × 109 / L), should determine whether cytopenia is associated with leukemia (extraction of bone marrow or biopsy). If cytopenia is not caused by leukemia, it is recommended that the dose should be reduced to 400 mg/day or 260 mg/m2/day for children and adolescents. If the blood cell reduction lasts for 2 weeks, further reduce the dose to 300mg/day or 200mg/m2/day for children and adolescents. If the blood cell reduction lasts for 4 weeks, the drug should be discontinued until neutrophils ≥1×109/L and platelet ≥ 20 × 109 / L. The re-use dose is 300 mg/day; or 200 mg/m2/day for children and adolescents. CML chronic phase and GIST patients (start dose 400mg / day or 260mg / m2 / day for children and adolescents): neutrophils <1.0 × 109 / L and / or platelets < 50 × 109 / L should be discontinued, in Medication should be resumed when neutrophils ≥1.5×109/L and platelets≥75×109/L, and the treatment can be restored to a dose of 400 mg/day or 260 mg/m2/day for children and adolescents. If the critical value reappears (neutrophils <1.0×109/L and/or platelets < 50×109/L), the retreatment dose after treatment interruption is reduced to 300 mg/day or 200 mg/m2/day for children and adolescents.
HES/CEL (starting dose 100 mg/day): When neutrophils ANC<1.0×109/L and/or platelets< 50×109/L should be discontinued, should be restored when neutrophils ANC≥1.5×109/L and platelets≥75×109/L Medication. Dosing can be re-dosed with the previous dose (ie, the dose before the serious adverse event occurred)
ASM (starting dose 100mg/day): When neutrophils ANC<1.0×109/L and/or platelets< 50×109/L should be discontinued, should be restored when neutrophils ANC≥1.5×109/L and platelets≥75×109/L Medication. Dosing can be resumed with the previous dose (ie, the dose before the serious adverse event occurred).
HES/CEL, ASM, MDS/MPD (starting dose 400 mg/day): When neutrophils <1.0×109/L and/or platelets< 50×109/L, the drug should be discontinued. When neutrophils ≥1.5×109/L and platelets≥75×109/L, the drug should be resumed. The retreatment dose was 400 mg/day. If the critical value occurs again (neutrophils <1.0×109/L and/or platelets<50×109/L), the retreatment dose should be reduced to 300 mg.
DFSP (dose 800mg / day) When neutrophils <1.0×109/L and/or platelets<50×109/L should be discontinued, the drug should be resumed when neutrophils ≥1.5×109/L and platelets≥75×109/L. The retreatment dose was 600 mg/day. If the critical value occurs again (neutrophils <1.0×109/L and/or platelets<50×109/L), the retreatment dose should be reduced to 400 mg.
Dose of patients with liver damage A mild dose of 400 mg/day is recommended for patients with mild to moderate liver damage. There are currently no data on patients with severe liver damage (more than three times of the normal range of bilirubin) using a dose of 400 mg/day. These patients should use this product after carefully weighing the risk assessment.
Dose of patients with renal failure Kidney clearance of imatinib is negligible. For this reason, it is expected that the systemic clearance rate in patients with impaired renal function is not reduced. However, special attention is still needed for patients with severe renal impairment.
Dose of elderly patients There are no special adjustment doses for elderly patients.
Note: Please refer to the product package insert for details. |
2013: First-to-market generic drug in China
2013: National Science and Technology Major Project
2013: Jiangsu Hi-Tech Product
2017: Included in NRDL